

Endothelin-1 (ET1) is a potent vasoconstrictor, mitogen, proinflammatory mediator, and a mediator of nociception, whose synthesis is increased by hypoxia, ischemia, shear stress, oxidative stress and reduced nitric oxide (NO) bioavailability, all of which are well documented mechanisms in the pathophysiology of sickle cell disease (SCD). We earlier reported on our studies on the role of ET-1 in SCD, and in transgenic mouse models showed that ETA receptor blockade with ambrisentan provides renal protection by preventing the development of glomerular hyperfiltration and proteinuria (Kasztan et al, 2017, Taylor et al, 2019, Kasztan and Pollock, 2019). ETA receptor blockade was also shown to decrease pulmonary inflammation in response to hypoxia/reoxygenation and LPS (Meiler et al.). Additionally, Lutz et al (2018) showed that pharmacologic inhibition or neuron specific knockdown of ETA receptor in primary sensory neurons of dorsal root ganglia in Berk mice alleviated basal and post-hypoxia evoked pain sensitivity. More recently (Kutlar et al, Blood 2019, 617,130036) we reported the preliminary results of a placebo controlled, double-blind phase I trial of ambrisentan in 26 subjects with SCD (SS and S-ß0 thalassemia) and microalbuminuria, and showed that the drug was well tolerated without any dose limiting toxicities and patients on ambrisentan had a reduction in microalbuminuria, especially in the subgroup who had been on concomitant ACEi/ARB therapy at a stable dose for at least six months (n=6, 286.1 mg/g Cr at baseline to 197.7 mg/g on day 85, p=0.06). FMD measurements showed increased arterial diameter, and improved microvascular function.
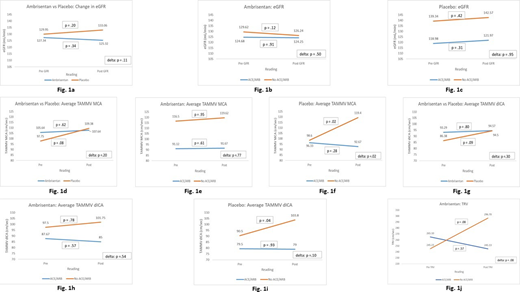
We analyzed data collected on secondary end points during the phase I study, including Tricuspid regurgitant jet velocity (TRV), Transcranial Doppler (TCD) velocities in distal internal carotid (dICA) and middle cerebral (MCA) arteries, and eGFR (calculated with CKD-Epi formula). Fig. 1a shows eGFRs in ambrisentan and placebo groups; Fig. 1b and Fig. 1c show a breakdown of ambrisentan and placebo groups based on concomitant ACEi/ARB usage. There is a reduction in glomerular hyperfiltration in the ambrisentan group compared to placebo, more pronounced in the subgroup who have not been on ACEi/ARBs. Fig. 1d depicts the change in flow velocity in MCA (TAMMV, Time Averaged Mean Maximal Velocity, cm/sec) between the ambrisentan and placebo groups; similarly, Fig. 1e and 1f show the breakdown of baseline and Day 85 TAMMVs in MCA according to ACEi/ARB usage. A similar trend is also observed in dICA flow (fig. 1g-1i), and suggests a synergistic effect of ETA receptor blockade with ACEi/ARBs in preventing an increase in blood flow velocities. TRV was available on 7 subjects, 6 of which were in the ambrisentan group. Fig. 1j shows the change in TRV in the ambrisentan group, and again is suggestive of a synergistic effect of ambrisentan and ACEi/ARBs in decreasing TRV. These data are clearly very preliminary, and are obtained on a small number of subjects, and as such, do not warrant any conclusions and or speculations. Nevertheless, an interesting observation is the apparent interaction of ETA receptor blockade and ACEi/ARBs in altering vascular flow/function in SCD patients. Decrease in microalbuminuria has been reported with ACEi and ARBs in SCD (Yee et al, 2018), without any effect on GFR. A reduction in hyperfiltration would likely have a significant renoprotective effect, at an earlier stage in the development of sickle nephropathy. ETA receptor antagonists are approved for the treatment of pulmonary arterial hypertension; thus, a decrease in TRV would have a beneficial effect. Increase in blood flow velocity in major intracranial vessels is a well established risk factor for ischemic stroke in children with SCD; however, much less is known in adults. In summary, the effect of ETA receptor blockade with or without ACEi/ARB, may have a significant effect on vascular function/blood flow in different organ systems, and should be explored in a large, multi-center phase II trial, with and without concomitant and or serial ACEi/ARBs, for a longer period of time, with a dose escalation, to further clarify the pleiotropic effects on multiple aspects of SCD pathology.
Kutlar:NIH/NHLBI (SCDIC): Research Funding; Global Blood Therapeutics: Research Funding, Speakers Bureau; Micelle Biopharma: Consultancy; Novartis Pharmaceuticals: Consultancy, Research Funding; Novo Nordisk: Research Funding; Forma Therapeutics: Research Funding; REACH: Other: DSMB Member; NOHARM: Other: DSMB Member; Bluebird Bio: Other: DSMB Member.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal